
Introduction to Sexuality
|
PART
I: Life's Greatest Miracle
For Part I you will be viewing the
PBS Nova Series "Life's Greatest Miracle. +Warning: There is a birth sequence at the end of this video which is really graphic (at about 54:00) Click HERE to go to "Life's Greatest Miracle." (Then click "Watch the Program.") |
|
|
Click on the following topics to read more about it:
|
|
Sexual Practices & Health Implications |
|
|
|
|
|
|
|
|
|



 (or “preference”) for sharing
sexual expression with members of the opposite
sex (heterosexuality), one’s own sex
(homosexuality), or both sexes (bisexuality).
(or “preference”) for sharing
sexual expression with members of the opposite
sex (heterosexuality), one’s own sex
(homosexuality), or both sexes (bisexuality).
 permitted or considered
appropriate on the basis of:
permitted or considered
appropriate on the basis of:
| Sexual Practices
and Their Health Implications
We would be remiss indeed if in a health class we did not discuss health risks of some of the common sexual practices.
Masturbation (manual or other non-penetrative stimulation of oneself or a partner for sexual pleasure)
Objects used to penetrate the rectum should be clean and nonbreakable, should have no sharp edges, and should not be shared with other people. Cover the object with a lubricated condom before it is used to penetrate the rectum. Do not insert the object too deeply into the rectum. Rarely, an object inserted in the rectum may break or may become lodged and cannot be retrieved. In these cases, medical help will be needed.
|
|
There are FIVE MAIN STAGES of the sexual response cycle: Stage 1: DESIRE
Indications of Desire: Desire is a prelude to sexual
excitement and sexual activity—it occurs in
the mind rather than the body and may not
progress to sexual excitement without further
physical or mental stimulation. Desire may be
communicated between potential sexual partners
either verbally or through body language and
behavior (for example, through “flirting”).
This communication, which is shaped by
sociocultural factors, may be subtle and
easily misread. In different cultures,
behaviors meant to communicate desire may vary
greatly along gender lines; for example, in
some cultures, women are expected not to
express overt, verbal communication of their
sexual desire, whereas such communication from
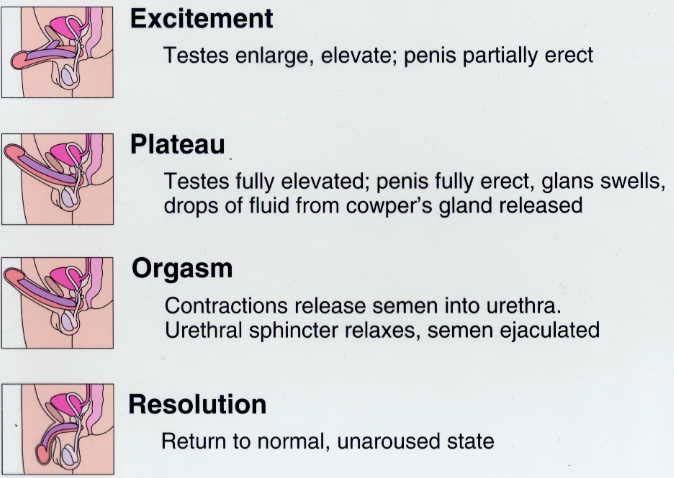
men is expected. Stage 2: EXCITEMENT (arousal)
Indications of Excitement: Excitement can be communicated between partners verbally, through body language, through behavior, or through any of the following body changes: * For both sexes: Heart rate
and blood pressure increase, body muscles
tense, sexual flush (reddening of the skin)
occurs, nipples become erect, genital and
pelvic blood vessels become engorged, and
involuntary and voluntary muscles contract.
The aroused person feels a sense of
restlessness. Stage 3: PLATEAU
Indications of the Plateau Stage: The plateau stage can be communicated between partners verbally, through body language, through behavior, or through any of the following physiological changes: * For both sexes: Breathing rate,
heart rate, and blood pressure further
increase, sexual flush deepens, and muscle
tension increases. There is a sense of
impending orgasm. Stage 4: ORGASM
Indications of Orgasm: The intensity of orgasm can vary among individuals and can vary for an individual from one sexual experience to another. Orgasm may involve intense spasm and loss of awareness, or it may be signaled by as little as a sigh or subtle relaxation. Orgasm can be communicated between partners verbally, through body language, through behavior, or through any of the following physiological changes: * For both sexes: Heart
rate, breathing, and blood pressure reach
their highest peak, sexual flush spreads over
the body, and there is a loss of muscle
control (spasms). Stage 5: RESOLUTION
Indications of Resolution: Resolution can be communicated between partners verbally, through body language, through behavior, or through any of the following body changes: * For both sexes: Heart rate
and blood pressure dip below normal, returning
to normal soon afterward; the whole body
(including the palms of hands and soles of
feet) sweats; there is a loss of muscle
tension, increased relaxation, and drowsiness.
MALE Sexual Response
|
|
|
"Sexuality MiniCourse by Engender Health" For more information, Click Here to view the entire minicourse. |
![]()